
By Dr Dominic Sparkes
In this blog, Dom shares his experiences of his Global Health Fellowship and reflects on how to move forwards from the pandemic.
Dominic joined CGHP as a Global Health Fellow in 2021. He is a Specialist Registrar in Infectious Diseases and Medical Microbiology joining Cambridge University Hospitals in 2018, he has previously worked in hospitals in London and Leeds. He has a keen interest in medical education and is working towards a PGCert in medical education.

Over the last six months, I have been working as a Global Health Fellow, this has been a wonderful opportunity. I have recently been reflecting on the challenges facing the partnerships, how they can progress further in the current climate of reduced travel due to the COVID-19 pandemic, and the use of technology to further them. Here I will outline the projects I have been working on, discuss the use of technology within the partnerships and my reflections on what this could mean for the future.
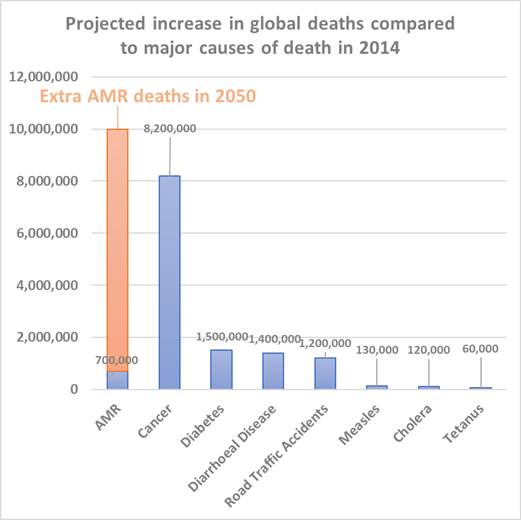
The first partnership is well established, between Kawempe National Referral Hospital (KNRH) and CUH, working to improve antibiotic stewardship (AMS) and infection prevention & control (IPC). By 2050 the rise of antimicrobial resistance is estimated to cause more deaths than cancer (figure 1), and there is a very real possibility that we will be living in a post antibiotic world, meaning some antibiotics will be ineffective against diseases.
We try to reduce this risk through AMS and good IPC practices. AMS involves ensuring the correct antibiotic is chosen for the correct duration and for the correct indication (presenting symptoms which indicate disease). The aim of this is to reduce the total amount of antibiotics used, reducing the selection pressure on bacteria and consequently reducing the opportunity to develop resistance. In contrast good IPC involves interventions to reduce the spread of infections, for example handwashing and appropriate patient isolation. This is beneficial to the individual to reduce the number of infections, but also reduces antibiotic use, and consequently antimicrobial resistance.
Earlier this year, the partnership team created educational videos which have been used as the basis of training sessions at KNRH. We have also attended regular meetings to support the setting up of a medicines technical committee to guide antibiotic prescribing plans.
Since March 2020 there has been an enormous increase in the use of different technologies to enable communication which has opened cross border discussions. Phrases such as, “shall we set up a Teams” or “lets Zoom” were previously reserved for the most technologically savvy but now is part of common parlance! We live in a world where face-to-face communication is available wherever there is an even vaguely stable internet connection. This has been hugely beneficial. We have been able to communicate with colleagues in Uganda regularly and work together effectively. Without the COVID-19 pandemic I do not believe we would have had these meetings; it is more likely we would have communicated ad hoc by email.
The use of technology has also been a key factor in the second partnership I have worked on. This is with colleagues working in Parirenyatwa Hospital, the teaching hospital of the University of Zimbabwe in Harare. This is also an educational partnership. We are working to support the development and modernisation of a Diploma in Sexual Health and HIV. The partnership team has created a regular educational meeting between CUH Infection Registrars and Post-graduate Medical Trainees in Parirenyatwa. These educational sessions are monthly case-based discussions, where an interesting case is presented by a trainee from each hospital with opportunity for discussion and key learning points to be established. This is held over Zoom and simply would not be possible without this technology.
As we come out of the latest wave of the pandemic a lot of society has reflected on the use of technology and how we work, resulting in a dramatic increase of remote working. There are obvious benefits to this, including but not limited to, reduction in commuting. This is both beneficial to an individual’s time, but also reduces the environmental impact. These new uses of technology are particularly useful when considering Global Partnerships. I strongly believe that although the use of technology has been fantastic and offered novel opportunities to further our partnerships, this cannot replace in-person visits. Such visits offer the opportunity to see areas for development for oneself but also, and arguably more importantly, the soft benefits of getting to know your colleagues better and bouncing ideas off each other. Moving forward for future iterations of Global Health Fellows, I think it will remain important to have visits to countries where the partnerships are held. When creating the often quoted ‘new normal’ we should not forget the benefits of how things worked pre-pandemic.
If you are interested in supporting CGHP, please follow the donate button below or contact the team.
Return to blogs