
By Millie Benjamin
In this blog, Global Health Fellow Millie Benjamin reflects on a visit to Uganda, as part of the Kampala-Cambridge partnership. Through strengthening clinical, diagnostic and laboratory capacity – as well as increasing understanding of antimicrobial resistance – the partnership working towards improving maternal and neonatal health.
Millie Benjamin is an ST3 Specialty Registrar in Infectious Diseases and Medical Microbiology, working in the East of England. She graduated in 2018 and has previously worked in hospitals in London. Millie has a particular interest in antimicrobial resistance and the development of effective antimicrobial stewardship (AMS) practices.
Find out more about all our current Global Health Fellows and their areas of expertise.

Background
Antimicrobial resistance (AMR) is a global public health and development threat of which we should all be aware. It is vital that we reduce the inappropriate use of antimicrobials and improve our antimicrobial stewardship (AMS) practices, to avoid the deeply concerning risks of death, disability, and economic strain that AMR poses to all of us.
Although AMR affects all countries and income levels, low-and-middle income countries are expected to shoulder a greater AMR burden. It is projected that if we do not make changes now, by 2030 up to 10 million deaths will occur annually due to AMR – with the majority in Africa and Asia (O’Neill, 2014). Uganda is one such country where the impact of AMR is expected to be felt.

Collecting GPPS data on the post-natal ward with the Kawempe Medicines and Therapeutics Committee.
The partnership
The Kampala-Cambridge AMS IPC partnership, supported by CGHP, was established in 2014. Prior to its set-up, AMR was identified as a key issue that was not specifically addressed locally or as part of the health partnership programme of activities. Therefore, following the COVID pandemic, infection prevention & control (IPC) and AMS were targeted as areas for development at Kawempe National Referral Hospital (KNRH). The 200-bed hospital is based in Kampala, Uganda, and is a government-funded women and children’s hospital, serving the Kampala Capital City Authority surrounding districts.
Through strengthening clinical, diagnostic and laboratory capacity, in addition to increasing understanding of AMR, the partnership has the overall goal of improving maternal and neonatal health.
On this visit and in this phase of the partnership, supported by funding from CwPAMS 2, our goal was to expand the delivery of AMS interventions already implemented at KNRH to four surrounding health centres (‘spoke’ sites), as part of a ‘hub and spoke’ model. These sites are local healthcare facilities that refer patients into KNRH, acting as crucial elements of a wider maternal healthcare network.
We also wanted to strengthen and expand the AMS work at KNRH, now the ‘hub’ site, and to gain a better understanding of the KNRH laboratory’s capacity. The development of local microbiological laboratory facilities will allow identification of resistance patterns in infection and promote targeted antimicrobial treatment.
The visit
I travelled with fellow Infectious diseases registrar Dr Suny Coscione, a 2022-2023 Global Health Fellow. After landing in Entebbe airport, we soon made our way to Kampala, where we were to stay for the next two weeks. As soon as we landed in Uganda, I found the people to be overwhelmingly kind and friendly. Kampala is an incredibly busy hive of activity; on the rare occasion we encountered it at a quiet moment, I found its vibrant colours strikingly beautiful.

A view of Kampala from Kawempe Hospital.
On our first full day, we were introduced to Dr Musa Sekikubo, consultant obstetrician and Uganda AMS IPC Partnership Lead, and Arnold Bababweyaka and Ronald Onegwa, who have both maintained key roles in the partnership since its initiation. We also met with the laboratory staff who we would come to work closely with over the next two weeks.
The days that followed saw us successfully conduct a Point Prevalence Survey (PPS), to establish the current antimicrobial consumption in KNRH. This including us supporting a training session of the Kawempe Medicines and Therapeutics Committee (MTC) on PPS methodology, followed by data collection on the post-natal and Neonatal ICU (NICU) wards. We collected data from 150 patients, and subsequently analysed this data and presented it to the MTC, in addition to generating a PPS report for the director of KNRH, Dr Emmanuel Byaruhanga.

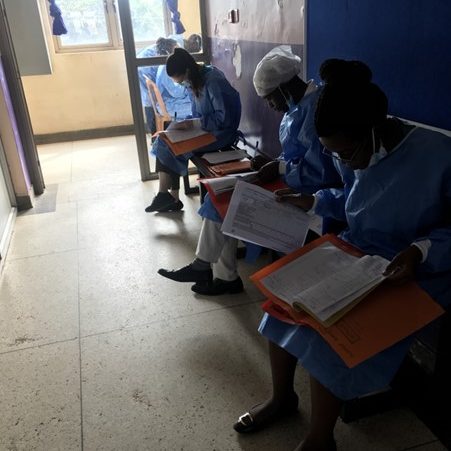
Preparing for and then collecting GPPS data on the post-natal ward with the MTC.
Over these few days we were also given the opportunity to gain an understanding of the current laboratory practices at KNRH, and the challenges that they frequently encounter when processing samples. We spent time speaking to laboratory staff and summarising the results of bacterial culture and sensitivity samples over the past three months. This enabled us to feed back to KNRH’s MTC and Dr Sekikubo on how the laboratory currently runs, and what changes may need to be made to increase their capacity.
The weekend that divided up our two-week visit meant that we were given the opportunity to explore Uganda a little more. Our Saturday was spent crossing Lake Victoria on a (somewhat!) rocky boat journey, over the Equator, to visit Ngamba Island Chimpanzee Sanctuary, just off the coast of Entebbe.

Crossing the Equator!
After a restful weekend, the next week was another busy one. The first two days involved visiting the four ‘spoke’ sites surrounding Kawempe Hospital, where we met with key members of each centre’s leadership team and introduced the AMS stewardship interventions we wanted to extend to their site. At each ‘spoke’ site we supported the team at KNRH to perform a baseline ‘needs’ assessment, to understand their current AMS and IPC activities, and the necessary support and training each of them will specifically require. We were then involved in feeding back the ‘needs’ assessment to Dr Sekikubo and other key members of the Kampala partnership and helped in devising a plan of action for the upcoming three months.
After an exhausting yet productive two weeks, it was time for our return to the UK. I am incredibly thankful for the opportunity to visit Uganda so early in my fellowship; the trip has most definitely inspired me to continue to build upon the AMS interventions work over the coming year.
Conclusions
- Antimicrobial consumption in KNRH (from the GPPS)
– Currently, 100% of antibiotic prescriptions are intravenous. We saw an opportunity to reduce intravenous antibiotic use by using oral formulations of antibiotics where possible. This will reduce expenditure, and free up more nursing time.
– Increasing the number of samples sent for microbiological testing would allow the transition from empirical to targeted antimicrobial prescribing. Currently, 100% antibiotic prescriptions were empirical, and only 2% of the total number of patients had had microbiological samples sent.
– Shorter durations of antibiotics may be introduced for some patients. All patients were prescribed three days of antibiotics following a Casearean section. However, there is increasing evidence that shorter durations of antibiotics for surgical prophylaxis, even single doses at the time of surgery, are as effective as longer durations. - Improving laboratory capacity
– From our time spent within the KNRH laboratory, we concluded that the lab can be supported to process more microbiological samples. The main reasons for too few samples being processed were a lack of a sustained supply of reagents required for sample processing, and clinicians not requesting microbiological tests because of this – along with difficulty in accessing the results. We suggested that the KNRH laboratory invest more funding in ensuring both the supply of reagents was constant, and in acquiring reliable materials. This will increase laboratory capacity, enabling more samples to be sent from hospital inpatients. In turn, antimicrobial prescriptions will be targeted rather than empirical, facilitating better AMS.
What’s next
Over the next few months, the Cambridge-Kampala partnership plans to:
- Feedback the results from the ‘needs’ assessment to each ‘spoke’ site.
- Deliver AMS training for ‘spoke’ site staff and facilitate the formation of an MTC at each site if not already formed.
- Conduct further training for pharmacists and interns at KNRH.
- Build upon KNRH’s current laboratory capacity.
We are fortunate that a second partnership visit is already confirmed for Spring, with both a microbiology trainee and a pharmacist visiting KNRH for three months between February-April. We are both looking forward to continuing to work with such a great team of people in 2024.
Return to blogs