By Topun Austin
Topun Austin, CGHP Member and Consultant Neonatologist at Cambridge University Hospitals NHS Foundation Trust, shares a deeply personal global health journey—from a formative medical elective in Nepal to a long-standing commitment to partnership working.
Thirty years after my medical elective in Kathmandu, I returned to find a changed country. Significant challenges remain in delivering neonatal care, but there is much we can learn from Nepal’s family-centred practice.
1994 – A transformative adventure

Ever since reading Tintin in Tibet as a child I was fascinated by the Himalayas, so when it came to my medical elective in 1994, Nepal was top of my list. Already drawn to neonatal medicine, I was introduced at University College London (UCL) to Professor Anthony Costello, who had spent two years in Baglung district in western Nepal, and through him to Dr Dharma Manandhar, director of the neonatal unit at Kathmandu’s largest government maternity hospital.
The UCL team was exploring a treatment for babies who were starved of oxygen at birth (hypoxic-ischaemic encephalopathy, HIE) and whether cooling babies might prevent brain injury; since Kathmandu sits at altitude they wondered if newborns there might cool spontaneously. The UCL department lent me a specialised ‘zero-heat flux’ thermometer that estimated deep body temperature using a simple sensor placed on the skin.
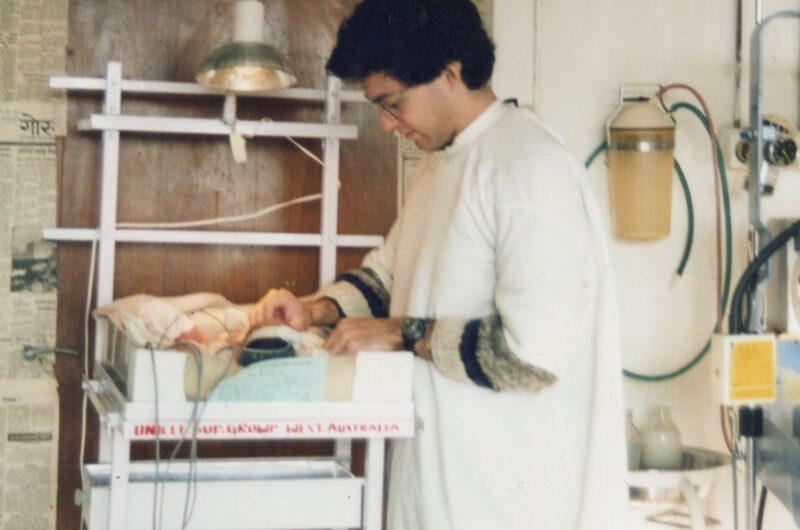
The three months that followed at Prasuti Griha Maternity Hospital were among the most formative of my career. Dr Manandhar was a visionary clinician who had built a remarkable unit on the principle that most babies survive with attention to the basics. Incubators were metal frames warmed by a spotlight bulb – 60 watts for a term baby, 100 for a preterm, 150 for the tiniest. Phototherapy was three babies sharing a basinet under blue-filtered strip lights. Cheap, but effective. Each morning he would autoclave his newspaper and hand it over:
“Dry your hands with this – you may get a bit of ink, but it is sterile!”
The lesson was that resource-appropriate basics benefit the majority of babies; there is no point in high-tech kit if you don’t get the basics right. The spotlights worked too well and my babies stayed warm. Cooling is now standard care for HIE in high-income countries, though the evidence base in settings like Nepal remains elusive.
2024 – Return to Nepal
In June 2024, I waved off my youngest son Arun at Heathrow airport on his own elective in Kathmandu. Regular FaceTime calls brought 1994 flooding back, and that autumn, while working in Singapore, I flew to Kathmandu to meet the new director of the renamed Paropakar Maternity Hospital.
The country had transformed: monarchy to republic in 2008, the 2015 earthquake, a steady drift of people into the valley. Where I had once cycled past the odd bus and stray dog, it was now impossible to move or breathe for the scooters. The neonatal unit had been transformed – familiar intensive and special care areas in place of metal frames and spotlights. Around 15,000 babies are born here each year (against 5,000 at the Rosie in Cambridge), all receiving free care (https://nepalitimes.com/prasuti-griha). The local healthcare practitioners I spoke with explained that only four nurses cover the 15 intensive and 25 special care cots between them. Despite this, mortality has fallen from four or five deaths a week to four or five a month, and babies as small as 700g and 27 weeks are surviving.

What was truly transformative was the kangaroo-care ward. Kangaroo mother care (KMC) – which promotes continuous skin-to-skin contact– maintains temperature, reduces oxygen requirement and promotes breastfeeding. A large trial in low- and middle-income countries showed a survival benefit from immediate KMC, prompting WHO to recommend it for 8–24 hours a day. In Kathmandu, babies as small as 1,200g go home fully breastfed; in the UK we would not dream of discharging such small infants, and preterm breastfeeding rates hover around 15%. Even more striking is the involvement of fathers – a cultural shift in a country where newborn care has traditionally fallen to women.


2025 – Making up for lost time
Back in Cambridge, I noticed my surgical colleague Anna-May Long wearing a Nepal lanyard. A shared history quickly emerged, leading us to Cambridge Global Health Partnerships (CGHP). Anna-May’s focus is gastroschisis, which carries a high mortality without proper management. In April 2025, I travelled back for a paediatric surgical conference run with the support of Anna-May and the British Association of Paediatric Surgeons.
In November that year, I returned for the third time in just over a year, for the Federation of Asian and Oceanic Perinatal Societies meeting. The keynote was given by Professor Costello, introduced by Professor Manandhar – now in his late 80s and as sharp as ever. A further visit to Paropakar opened conversations about developing a teaching programme, and a possible elective exchange for medical students. With the support of CGHP, preparations are being made to run a course on newborn brain imaging and monitoring to support some of the most vulnerable of the 15000 babies born at Paropakar each year. Alongside this training, there are plans to enable nurses in the UK to learn from colleagues in Nepal—particularly in the delivery of KMC, where Nepal’s experience offers valuable insights for improving neonatal outcomes.


Postscript

Nepal is a magical country. Once you climb out of the Kathmandu smog, the Himalayas rear into the sky – the home of the gods. With tourism a fickle main export and the corruption that fuelled the ‘Gen-Z revolution’ of October 2025, Nepal remains one of the world’s poorest countries. But as Dr Karmacharya said to me, “once a baby cries, they have a right to survive” – and that is true wherever in the world you are born.
If you’d like to make a donation to support this partnership and help improve outcomes for some of the most vulnerable newborns, please get in touch with our team at info@cghp.org.uk
References:
- WHO Immediate KMC Study Group; Immediate “Kangaroo Mother Care” and Survival of Infants with Low Birth Weight. N Engl J Med. 2021 May 27;384(21):2028-2038. doi: 10.1056/NEJMoa2026486.
- Levene I, et al. Breastfeeding trajectories for preterm infants over the first 6 months of life in England 2010-2020: surveys using large representative birth samples. BMJ Paediatr Open. 2024 Oct 21;8(1):e002912. doi: 10.1136/bmjpo-2024-002912.
Return to blogs